How to Cite the Institute of Medicine Redesigning Continuing Education in the Health Professions
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
3
Regulation and Financing
Regulation and financing are critical components of continuing education (CE). The regulation of CE is arguably intended to be a proxy for quality, as it establishes a minimum set of quality standards, while the financing pays for the conduct and research of CE activities. However, regulatory and financing mechanisms for CE are disconnected from and poorly aligned with the goals of improving health professionals' performance. Little uniformity exists in CE regulation and financing across health professions, inhibiting development of a modern, integrated, team-oriented workforce. This chapter explores regulation and financing of continuing education in the largest sectors of the health care workforce—medicine, nursing, pharmacy, and social work.1
REGULATION OF CONTINUING EDUCATION IN SELECT HEALTH PROFESSIONS
The current regulation of CE attempts to ensure high quality learning for health professionals by targeting individual professionals through licensure, certification, and credentialing, and by targeting providers of learning activities through accreditation. As
| 1 | These are the largest professions as measured by numbers of professionals, with more than 200,000 clinicians. The committee recognizes the various health professions identified in Appendix B but was unable to describe each profession in depth. |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
is the case with most other aspects of health care, each profession approaches regulation differently, using variable terminology and approaches to CE, employing different learning requirements, and developing unique regulatory processes.
Regulating Individual Health Professionals
Since the early 1970s, CE for health professionals has been linked directly to licensure, certification, and credentialing. The various regulatory authorities—states for licensure, specialty societies for certification, and health care organizations for credentialing—attempt to ensure that a given health professional's background meets some minimal standard of quality.
Learning tools such as self-assessment, peer evaluation, and learning portfolios should all have a role in supporting the acquisition of knowledge and skills, reinforcing competence, and reassuring the public's trust (Cooke et al., 2006). However, current licensing and certification systems principally assess learning only by measuring health professionals' participation in CE. Despite some professions' efforts to recognize achievement in knowledge, competence, and performance (Miller et al., 2008), the systems are still strongly linked to participation and not specifically focused on measures that really matter—changes in professional behavior and patient outcomes.
Licensure
In many health professions, professionals are mandated by law to receive a license to practice from a state licensing board (Mazmanian et al., 1979), and health professionals may hold a license in more than one state. This requirement is arguably the strongest regulatory tool available to assess individual health professionals. However, licensure has been linked only tangentially to performance improvement (Davis et al., 2003). Moreover, while initial licensure establishes the minimum competence required for admission to a profession, it does not guarantee that a health professional will maintain competency or provide a high level of care.
Many states call for health professionals to apply for periodic relicensure, which often requires varying amounts of CE credits or hours. Requirements differ greatly by state and by health profession (see Figure 3-1). The various professional state boards are represented by national organizations, such as the Federation of State Medical Boards and the National Council of State Boards of Nursing. CE licensure requirements are generally organized around
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
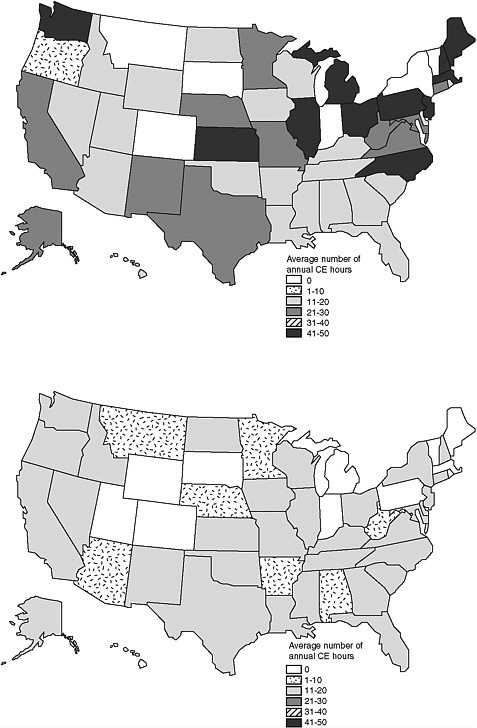
FIGURE 3-1 Average number of annual CE hours for physicians (M.D.s) (top) compared with physical therapists (bottom).
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
TABLE 3-1 Examples of CME Activities by Category
| Category 1 | Category 2 |
| Publishing articles | Consultation with peers |
| Poster presentations | Small-group discussion |
| Medically related advanced degrees | Self-assessment activities |
| Independent learning | Medical writing |
| Live or attendance-based activities | Teaching residents |
| Journal reading a | |
| a Journal reading is counted for Category 1 credit only when providers (i.e., journals) incorporate mechanisms for reflection and/or interaction with the article content. This requirement can be met through an evaluation or examination that physicians return to the provider. | |
learning activities that often are conducted in groups, such as at conferences and lectures, and the content and processes of learning are under the control of the CE provider. Licensure has been linked only tangentially to performance improvement (Davis et al., 2003).
Often, licensure and relicensure require certain amounts of particular types of CE activities, which are divided into "formal" and "informal" categories. For example, in medicine, these categories refer to Category 1 and Category 2™, defined and trademarked by the American Medical Association (2006) (see Table 3-1). To meet continuing medical education (CME) licensure and relicensure requirements, physicians must participate in a specified number of Category 1 and Category 2 activities, but only Category 1 activities count toward the required number of credits. The relative benefit of Category 1 over Category 2 activities is questionable, however, because some learning methods appear more effective than others, as discussed in Chapter 2. For example, self-assessment, a Category 2 activity, often imparts more lasting knowledge retention than a lecture, a Category 1 activity. Thus, the typical emphasis placed on providing and obtaining Category 1 credits may divert limited resources from more effective Category 2 activities.
Certification
Certification is the process by which professional specialty societies or credentialing bodies—not regulatory bodies—certify individual health professionals as qualified experts to practice in a particular area of a profession. In professions that require certification, such as medicine (under specialty boards), professionals must regularly repeat the certification processes, which differ by profes-
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
sion and by specialty. The American Board of Medical Specialties has recently adopted new standards for a four-component mandatory maintenance-of-certification program: the components focus on professional standing, lifelong learning and self-assessment, cognitive expertise, and evaluation of performance in practice. Instead of recertification being required once every 10 years, this shift toward a new type of maintenance of certification requires continual engagement in professional development (ABMS, 2009).
Credentialing
Credentialing occurs at the level of health care organizations, such as hospitals and group practices, that employ health professionals. Organizations use credentialing in an attempt to ensure that health professionals are qualified to practice and maintain a minimum level of competence and performance. Many organizations use credentialing as the basis for granting staff privileges, and some organizations also credential health professionals for particular procedures, based on their experience and clinical outcomes. Many organizations develop their own credentialing guidelines. The process can be likened to an audit. Credentialing often includes, at a minimum, review and verification of a health professional's licensure, education, and certification, if applicable.
Examples of Fragmentation in Select Health Professions
The variation in the numbers of required CE credits (see Figure 3-1) and the content of such learning exemplifies the fragmentation in the current state of CE (see Table 3-2). Among the problems that such variation causes, current CE does not generally promote team-based learning. For example, health professionals do not normally learn with clinicians from other professions, partially as a result of disconnected and dissimilar CE systems. Health professionals from one profession also typically cannot earn CE credit for attending an activity offered by another profession, regardless of the degree to which the content may overlap and the relationships may foster collaborative practice.
Regulatory variations also result in some types of health professionals receiving more continuing education than others. For example, nurses are required to take only 5 hours of CE annually in one state and 15 hours in others. The picture is similar for pharmacists; some states require them to receive 10-60 credits per year to remain licensed, while some states have no CE requirements. In other pro-
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
TABLE 3-2 Comparison of CE Providers, Activities, Requirements, and Consequences of Failing to Meet Those Requirements in Four Health Professions
| Health Profession | Types of CE Providers |
| Medicine |
|
| Nursing |
|
| Pharmacy |
|
| Social Work |
|
| a Range is given for jurisdictions that require CE, because some states do not require CE in all professions. b Activities include seminars, workshops, teaching activities, course preparation, web-based courses, self-study experiences, and professional publication. | |
fessions, some states require that CE credits be taken in specific areas, such as HIV/AIDS and domestic violence, according to the profession. Certification requirements also differ by individual specialty boards. Increasingly, hospitals, insurers, and even partners in clinical practice require varying amounts and types of CE activities (Peck, 2000).
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
| Examples of Accredited CE Activities | CE Required per Year a | Repercussions for Failing to Receive CE |
| 10-75 CME credits |
|
| 5-15 contact hours |
|
| 10-60 CPE hours |
|
| 3-25 CE hours |
|
Regulation in social work is particularly variable; for example, states differ greatly in how they establish licensure categories and what titles they confer. Various licenses (e.g., licensed clinical social worker, licensed social worker, licensed graduate social worker) can be accompanied by vastly different requirements. Among states that mandate CE for licensure of social workers, requirements range
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
from 9 hours every 3 years to 50 hours every 2 years. While state board requirements vary, the National Association of Social Workers (NASW, 2003) has developed a separate, voluntary set of standards for CE that requires social workers to complete 48 hours of CE every 2 years to be recognized at the national level.
If health professionals fail to fulfill CE requirements, various degrees of repercussions and disciplinary action occur. Generally, health professionals are fined or suspended, and they may face revocation of licensure or credentialing, higher medical liability premiums, or loss of membership in professional and provider organizations. In nursing and other professions, a lapse in CE participation may be reported to state and federal data banks.
Many state boards conduct random audits of individual professionals to verify that they indeed completed their required CE activities. The Oregon State Board of Nursing, for example, audits a certain percentage of applicants for relicensure each month by requesting copies of CE certificates of completion (Grossman, 1998), and many state medical boards audit 1-25 percent of physicians per year to check whether they completed required CME activities (AMA, 2008).
However, not all health professions require ongoing licensure, certification, or credentialing. Many allied health professions' professional competency requirements are minimal beyond initial licensure and certification, and professionals are not required to relicense or recertify. For example, until recently, a licensed physical therapist was "entitled to practice indefinitely" (Brosky and Scott, 2007). Defining, assessing, and measuring ongoing professional competence in physical therapy has recently garnered attention, as the profession has become more autonomous (as exemplified by direct access to patients without a referral) and the doctor of physical therapy has become the entry-level degree.
Consistent Licensure, Certification, and Credentialing
Licensure, certification, and credentialing need to become more consistent, and standardized requirements need to be established, to help ensure minimal levels of competence. Efforts to align these processes have begun to occur in small pockets. For example, the nursing community is moving toward greater unanimity around CE requirements for licensure across states. Therefore, licensure, certification, and credentialing ought to reward improvement of competence, performance, and patient health, instead of focusing merely on rewarding skills, as is now the case.
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
It will be important for the regulatory system to recognize the inextricable linkage between the continuing education of all health care professionals and health care teams, the quality of patient care, and the quality of system performance. This will require developing linkages among the various regulators of health care and developing new standards and processes. Today's simple credit system, which reinforces the isolated "silo" structure that characterizes regulatory activities, should be abandoned. The organizations involved in regulation should work together to define the purposes of regulations and the areas on which regulators should focus. Standards should be developed that attend to the linkages in ways that reinforce the work of each regulatory system. Action needs to be taken to foster and publicly recognize team-based, local, and national learning about good regulation and good health care.
Licensure and certification processes should reward successful demonstration of maintenance of competence. Additionally, certification should require a minimum standard of practice-based learning to promote the identification and solution of practice-based needs. To promote reflection, licensure or credentialing should require demonstrated use of learning portfolios with documented needs assessments. Learning activities should be granted licensure or credentialing only if they have demonstrated effectiveness for improving professionals' learning or performance, or for improving patient outcomes.
Accreditation of CE Providers in Select Health Professions
Accredited CE providers include organizations such as hospital systems, professional membership and specialty organizations, publishing/education companies, professional schools, and, in some cases, state boards. Accreditation bodies generally conduct formal accreditation processes at both regional and national levels. Accreditation attempts to confirm the quality and integrity of accredited CE by establishing criteria for the evaluation of the providers, assessing whether accredited providers meet and maintain minimum standards, and promoting provider self-assessment and improvement (Michigan State Medical Society Committee on CME Accreditation, 2009). Accreditation bodies evolved as an effort to assure the professions and the public of the quality of teaching and education in the health professions. Box 3-1 provides an example of the development of the Accreditation Council for Continuing Medical Education (ACCME).
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
BOX 3-1
History: Development of the ACCME
Continuing medical education (CME) in the United States includes a long history of American Medical Association (AMA) initiatives to acknowledge physicians' participation in CME and to approve state medical societies as accreditors of regional CME programs. In 1968, the AMA developed the Physician's Recognition Award (AMA/PRA), which is awarded to physicians who participate in 150 hours or more of CME during a 3-year period. In 1971, the AMA decided that only courses offered by organizations accredited by the AMA Council on Medical Education would count toward the award.
As demands grew to make participation in CME mandatory for medical relicensure, professional society memberships, specialty certification, and credentialing, the AMA Council on Medical Education delegated select accreditation tasks to local or regional organizations, including state medical societies. In 1977, the AMA helped to initiate the Liaison Committee on Continuing Medical Education (LCCME), which assumed the accreditation role previously held by the AMA Council on Medical Education. The LCCME and its successor, the Accreditation Council for Continuing Medical Education (ACCME), included various participation. a The ACCME currently serves as the body that accredits institutions and organizations nationally to offering CME and to designating Category 1 credit, and recognizes institutions and organizations, including state medical societies, to confer CME accreditation that enables the designation of Category 1 credit for qualified CME activities.
| a Participants included the AMA, American Board of Medical Specialties, American Hospital Association, Association for Hospital Medical Education, Association of American Medical Colleges, Council of Medical Specialty Societies, and Federation of State Medical Boards. |
Current State of Accreditation
Depending on the profession, some accreditors review the quality of specific CE activities and programs, while others attempt to assess CE providers themselves. Entities wishing to provide CE may voluntarily pursue accreditation. In granting accreditation, accreditors look for such things as whether the CE provider provides a written mission statement reflecting the values and ethics of the profession and whether it will assist professionals in maintaining and enhancing professional competencies to practice in various settings. As an example of such efforts, the criteria used by the American Nurses Credentialing Center (ANCC) are listed in Box 3-2. Additionally, each profession has developed specific regulations regarding
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
BOX 3-2
Example of Accreditation Criteria
The American Nurses Credentialing Center, a major national accreditation body for continuing nursing education (CNE), defines the following criteria for provider accreditation:
-
CNE must be conducted by accredited "provider units," which should document that the organizations' beliefs and goals are relevant and appropriate to prospective learners;
-
CNE activities must be tailored to the educational needs of the target audience;
-
Each educational activity must be planned by groups with the relevant content expertise and representation from the target audience;
-
Each CNE activity must be designed with an identified purpose and learner objectives, content and teaching strategies to achieve the objectives, and criteria for completion of the CE activity; and
-
Each CNE activity must include an evaluative measure that includes learner input and a method for verifying that participation in the activity occurred.
conflicts of interest and commercial support for CE activities and providers.
CE providers can apply for an accreditation period of 4-6 years in many health professions (e.g., medicine, nursing, pharmacy). The accreditation process requires ongoing evaluation and improvement processes and contact with providers. For example, in medicine, the ACCME calls on a group of more than 150 volunteers to interview providers applying for reaccreditation and requires providers to submit an annual report describing the size and scope of activities planned and executed. The ANCC conducts site visits of continuing nursing education (CNE) providers to ensure their quality; those that do not adhere to requirements can have their accreditation suspended or revoked (ANCC, 2009).
In pharmacy, pharmaceutical manufacturers directly provide continuing education, but these CE providers must plan all activities independent of commercial interests and present their materials to participants with full disclosure of manufacturer participation and sufficient balance. Social work associations in certain states also accredit CE providers; many states do not require preapproval of CE providers, but instead depend on the social workers they
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
license to ensure that CE activities comply with state administrative requirements.
Consistent Accreditation
Establishing consistent accreditation standards across professions and states would have a number of advantages. Standardization would allow the already underresourced accreditation infrastructure to be streamlined around common procedures. It would also reduce the potential for programs that have been declined accreditation by one agency to take advantage of lenient accreditation standards elsewhere, and it would promote a system of sharing best practices, as other accreditors could apply similar standards. Standardized accreditation requirements would become the expectation of learners, allowing learners to more easily identify deviations from the norm. Consistent accreditation requirements adopted across professions would facilitate interprofessional education in CE because providers would accredit their courses for multiple types of health professionals who would learn together.
FINANCING OF CONTINUING EDUCATION 2
Financing is an overarching issue in any discussion of CE because innovations in learning require that teachers, students, and organizations have the necessary resources for learning (Cooke et al., 2006). The financing of CE, as with its regulation, varies by profession. Table 3-3 provides an overview of CE financing in medicine.
CE Providers
Continuing education is provided by many different entities. A complete breakdown is not available for all health professions, but Figure 3-2 shows CE providers in medicine. Medical schools provide the most hours of continuing medical education (45 percent of the total). Professional societies and organizations provide nearly a quarter of all CME hours, and they also are important providers outside of medicine (ACCME, 2008). Employers of health care professionals, such as the Department of Veterans Affairs (VA), and health
| 2 | The best estimate of financing in CE available for this analysis was from the ACCME Annual Report Data, which provides information only in medicine. Therefore, this section focuses mainly on financing in medicine but may have implications for other health professions. |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
TABLE 3-3 Overview of Current CE Financing in Medicine
| Current System | |
| Industry funding? | Yes, ~58% of total |
| Out-of-pocket cost to physicians | ~42% of total, or $1,200 per physician per year |
| Mode of delivery | Primarily in-person lectures and workshops, with a small amount of simulation training and performance improvement exercises taking hold |
| Educational value, impact on patient care | Unclear |
care institutions, such as hospitals and insurers, may also provide continuing education. Particularly in medicine and pharmacy, commercial CE institutions are important providers of CE.
Commercial entities include medical education and communication companies (MECCs), which are generally for-profit companies hired by commercial interests to organize meetings, find speakers for conferences or lectures, and develop enduring materials (Coogle, 2008; Steinbrook, 2005). A 2007 quantitative survey of 79 MECCs found that 53 percent reported being part of a larger organization that included companies involved in commercial promotion (Peterson et al., 2008). Even though many commercial companies are accredited by the ACCME, their motivations have sometimes been questioned due to the potential bias they introduce and the volume of CE they provide (Blumenthal, 2004; Brennan et al., 2006; DeAngelis and Fontanarosa, 2008; United States Senate Committee on Finance, 2007).
Cost of CME
Data on the costs of CE outside medicine are limited. In 2007, the total cost of CME provided at a national level was $2.54 billion, consisting of commercial support, advertising and exhibit income, and registration fees and other income. On average, ACCME providers generated profits of 23.5 percent, as shown in Table 3-4. Professional societies derived the largest profit margins (31.8 percent). Publishing/education companies, which include but are not exclu-
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
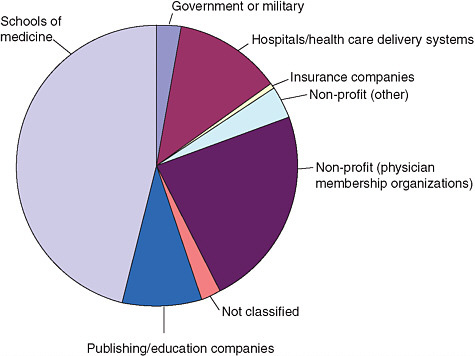
FIGURE 3-2 Hours of directly sponsored CME by organization type.
SOURCE: ACCME, 2008.
sively composed of MECCs, derived 25.9 percent profit margins (ACCME, 2008).
Who Pays for CE?
Financing of CE varies by profession. Some health professionals pay out of pocket for their CE, while employers, commercial entities, and others may pay for all or part of the continued learning expenses of other professionals. Thus, CE funding comes from numerous sources, including health professionals themselves, employers, commercial entities, and the government.
In many health professions, including occupational therapy and dentistry, health professionals are generally responsible for paying for a majority of their own CE. This culture of paying out of pocket for CE closely resembles the culture in other industries (e.g., certified public accountants). When the costs are borne by individuals, they are likely to choose an activity based on its perceived value, which may, however, be based more on the activity's cost and convenience than its content and clinical benefit. In 2007, physicians paid 42
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
percent ($1.05 billion) of the total $2.54 billion spent on CME. On average, a physician paid slightly more than $1,400 per year for his CME.3 Data on the costs of CE paid by individual health professionals in each profession were unavailable for this assessment.
Some organizations see continuing education as an investment in staff development and bear at least a portion of CE costs. The opportunity costs of lost staff time, as well as the fees and other costs associated with an activity, may, however, be seen as a drain on health care organizations in times of shrinking financial resources.
The federal government provides little direct financing for CE for health professionals, especially compared with the billions of dollars of public support for graduate and undergraduate education. Public funds are used, for example, toward the CE of professionals sponsored by the VA, the Department of Defense, and the Indian Health Service. Some other federal funds support CE activities. For example, the Health Resources and Services Administration provides some funding for health professions CE through Titles VII and VIII of the Public Health Service Act. No consistent investment for a large majority of nongovernment-related health professionals exists.
Particularly in medicine and pharmacy (and nursing to a lesser extent), funding for CE also comes through direct funding of CE providers from a variety of sources, including employers, professional societies, and commercial entities.
Issues Around Funding and Provision of CE
Two current features of CE funding may inhibit achievement of better CE. One concern arises because of the role of commercial funding and the conflicts of interest that may result. A second concern is that the silo structure of many professional organizations and education institutions may inhibit learning and interprofessional collaboration.
| 3 | The total income into the CME system ($2.54 billion) was the minuend from which the total commercial support ($1.5 billion) was subtracted. The difference ($1.04 billion) was presumed by the researchers to be the amount paid out of pocket by physicians. This figure was divided by 718,000, the approximate number of active physicians (not including residents and fellows) in the United States in 2007 (personal communication, J. Cultice, Health Resources and Services Administration, May 27, 2009). The resulting figure was taken to be a rough estimate of the out-of-pocket cost per physician per year. |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
TABLE 3-4 Financial Support of CME for Different Types of Organizations, 2007
| Organization Type | Number | Total Income | Commercial Support |
| Government or military | 15 | $69.5 million | $0.25 million (<0.5%) |
| Hospital or health care delivery system | 93 | $105 million | $47.5 million (45.2%) |
| Insurance company or managed care | 14 | $3.49 million | $0.32 million (9.2%) |
| Nonprofit (other) | 38 | $160.4 million | $78.4 million (48.9%) |
| Nonprofit (physician member organization) | 270 | $887.2 million | $215.4 million (24.3%) |
| Not classified | 33 | $55.2 million | $29.3 million (53.1%) |
| Publishing or education company | 150 | $830.8 million | $594.4 million (71.5%) |
| School of medicine | 123 | $427.7 million | $245.8 million (57.5%) |
| Total | 736 | $2.54 billion | $1.21 billion (47.7%) |
| SOURCE: ACCME, 2008. | |||
Conflict of Interest
Medically related industries, such as pharmaceutical and medical device companies, have taken a lead role in financing the research on and provision of CE in medicine and pharmacy, despite much controversy (Peterson et al., 2008). Since the 1960s, the dependence of CE on commercial funds has raised concerns about bias and conflicts of interest with respect to companies using CE as a means of inappropriately influencing health professionals, especially physicians, to increase their market shares (Podolsky and Greene, 2008). The first published empirical evidence found that approximately 43 percent of CE programs for pharmacists received commercial support, and that such high levels of support helped to create a culture
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
| Advertising and Exhibit Income | Registration Fees and Other Income | Total Expense | Profit Margin (%) |
| $0.38 million (0.55%) | $68.8 million (99.0%) | $69.2 million | 0.4 |
| $7.4 million (7.0%) | $50.1 million (47.7%) | $100.3 million | 4.5 |
| $0.035 million (1.0%) | $3.14 million (90.0%) | $6.72 million | −92.6 |
| $11.9 million (7.4%) | $70.1 million (43.7%) | $126.5 million | 21.1 |
| $217.9 million (24.6%) | $453.9 million (51.2%) | $605.3 million | 31.8 |
| $2.4 million (4.3%) | $23.5 million (42.6%) | $43.7 million | 20.8 |
| $10.8 million (1.3%) | $225.6 million (27.2%) | $615.7 million | 25.9 |
| $23.2 million (5.4%) | $158.7 million (37.1) | $375.8 million | 12.1 |
| $274.0 million (10.8%) | $1.05 billion (41.5%) | $1.94 billion | 23.6 |
in which pharmacists expect to obtain CE at a minimal cost and CE providers "are dependent on industry to assist them in covering administrative, educational, and noneducational expenses" (Smith et al., 2006, p. 310).
In 2007, $1.5 billion4 of CME funding came from commercial entities. Some efforts have been made to develop safeguards meant to ensure that CE providers are free from conflicts of interest. Yet widespread skepticism remains as to CE funders' intentions
| 4 | The total commercial support listed in the ACCME Annual Report Data (2008) is $1.21 billion; convention also adds the amount spent on advertising and exhibits income, $275 million, to derive the more complete $1.5 billion in commercial support. |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
(DeAngelis and Fontanarosa, 2008; Peterson et al., 2008; Relman, 2001; Steinbrook, 2008). The Institute of Medicine (IOM) Committee on Conflict of Interest in Medical Research, Education, and Practice has addressed these issues in depth and has recommended, among other things, that industry should not influence CME (IOM, 2009).
It is important to note that MECCs and other conflicted sources5 can be significant resources, for example, by supplying well-trained staff who provide high quality CE. Also, significant progress has been made in the past 5 years toward protecting educational content from potentially corrupting influences and promotional intent (ACCME, 2006; PhRMA, 2008). As in other health professions, the ACCME has detailed regulations to ensure that commercial interests are kept separate from learning activities and course content. The regulations require CME providers to disclose conflicts of interest and resolve relevant financial relationships with any commercial interest among those in a position to control CME content. For example, the ACCME requires CME providers to give a balanced view of therapeutic options and encourages the use of generic names of therapies, rather than promoting specific proprietary names (ACCME, 2006). Still, such efforts may not be sufficient to keep activities free from bias. For example, in some CME activities, conflicted sources are alleged to have planted members in audiences to ask specific questions about a particular drug, ensuring that the discussion will include that drug (McCartney, 2004). To monitor bias in CME, the ACCME requires providers to survey participants about potential commercial bias at the conclusion of events. Participants, however, may not necessarily be the best detectors of this bias (Steinbrook, 2005). The committee concludes that CE should be free of influence from conflicts of interest to protect the integrity of health professional development.
Interprofessional Collaboration
Although professional societies and organizations have important roles to play in continuing education, they also may be the sources of some problems. For example, their influence may be counter-productive to interprofessional collaboration, standards of certification, and patient care if they focus too narrowly on profession-specific interests and not on the best ways to improve health. Professional
| 5 | In the context of this report, conflicted sources are those that use CE primarily as a mechanism for advertising and marketing for their own personal or corporate gain and not for the continued improvement of health care quality and patient safety. |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
societies also may have potential conflicts of interest between their roles as protectors of the profession and providers of the learning that will drive collective competence. The roles of professional organizations need to explicitly include jointly fostering interprofessional education, promoting appropriate evidence-based approaches, and supporting lifelong learning. Checks and balances will be needed to ensure that professional societies are meeting all of these obligations appropriately.
Future Financing for a More Comprehensive System
Whether continuing education for health professionals should be financed by government, industry, employers, or individuals is still being debated. What is clear, however, is that funding should be directly aligned with the goals of driving improved quality of care and patient safety and should support a mix of activities that are effective both in terms of performance and cost. In this way, funding will help in developing a more comprehensive, broad-based system for professional development, called continuing professional development (CPD), as described in Chapter 1. In addition, strong safeguards need to be put in place to avert the development of education solely for the sake of profit, thus protecting the integrity of the system.
This shift of focus and priorities will almost certainly have implications for the amount of support available for CPD and its sources. Sources of CPD funding are unlikely to remain static because a market for CPD exists. As some sources disappear, new ones will likely emerge. To be responsive to changes in the field and the rapidly changing needs of the health professions, flexibility will be a necessary attribute of CPD funding structures.
Some commercial supporters are already looking past short-term, profit-driven CE toward funding programs that have the most impact on physician performance (Saxton, 2009). Figure 3-3 explores the intersection of areas of "business needs," "healthcare system quality gaps," "healthcare provider performance gaps," and "patient needs." This portrayal suggests that industry support could be of greatest value for all stakeholders at this intersection, if the purpose of the activity is to improve quality and patient safety. To identify the areas where industry needs and funding could align with the needs of the health care system, an effective research enterprise will have to be in place to identify gaps in the current system and to develop theories and effective interventions to fill them.
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
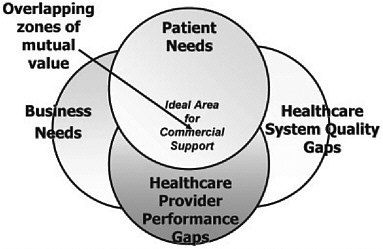
FIGURE 3-3 A convergence-of-interest model of commercial support.
SOURCE: Saxton, 2009.
The availability of industry funding has the potential to influence the types of CE programs offered. Currently, if alignment with industry interests determines the content of continuing education, areas of health care and patient safety that fall outside of industry interests generally receive less support. For example, if industry only funds therapeutics that are based in medications, these topics will be of greater priority for CE providers but may not be more effective in yielding better outcomes than other types of CE. This is inconsistent with a system of learner-driven CPD and needs to be remedied in the development of a new model of CPD funding.
One interesting question to ask is, what might happen if commercial funding were entirely withdrawn and no subsidies were provided by other sources? The average physician could fund his own CME and continue attending the same types of CME activities by investing about $3,500 annually.6 Although this is a rough estimate and does not take into account the nuances of the various sources of CME funding, it provides a general sense of how
| 6 | The figure is calculated by dividing $2.54 billion by 718,000 physicians, the number of active physicians (not including residents or fellows) in 2007 as reported by the Health Resources and Services Administration from the American Medical Association Physician Masterfile (personal communication, J. Cultice, Health Resources and Services Administration, May 27, 2009). A recent article estimates $4,013 spent per physician in 2007, based on a denominator of 633,000 physicians, a figure reported by the U.S. Bureau of Labor Statistics for physicians and surgeons in 2006 (Mazmanian, 2009). |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
much CME would cost. Without funding from conflicted sources, CE content would likely shift away from knowledge about specific drugs and devices. It is not clear, though, precisely how the content would change in the event conflicted funding sources disappeared because the content and types of CE that are biased and sponsored by conflicted sources is not well-defined. Also, it is important to understand that under such circumstances, CME providers may also change the amount and types of CE activities they sponsor.
Even if CME did not change, physicians could continue to fulfill existing regulatory CME requirements without increasing their out-of-pocket spending. For example, through journals such as the New England Journal of Medicine and the Journal of the American Medical Association, a physician can fulfill Category 1 regulatory requirements by paying approximately $150-$750 for an entire year's worth of 50 credits. These examples demonstrate how regulatory requirements can be satisfied while spending less than the average physician currently spends on CME. However, it is unlikely that all physicians would choose to adopt only low-cost, convenient CME, because they would likely be motivated to network and learn in part through other methods, such as live activities. In the event a credit-based system is used, regulatory and quasi-regulatory bodies could also place restrictions on the types of CME for which physicians can receive credit, ensuring that they receive CE credits through a variety of methods tailored to the specific learning needs and contexts.
Since not all physicians would choose the lowest-cost, most convenient methods, a medium-cost CME option might assume that physicians participate in CME not only to fulfill CME requirements but also to prepare for periodic recertification exams. Exam-preparatory CME would cost approximately $550 per physician per year.7 As in the journal-based CME option, many physicians would likely desire and choose to participate in higher quality, interactive CME events to network, update, and maintain their knowledge base. Physicians could fulfill most CME requirements by using inexpensive methods and spending less than they do now, leaving funds to attend some higher-cost, higher-value CME events. Therefore, a mix of cost-effective CE could be achievable in the current financing
| 7 | The average annual cost of recertification, calculated from the following medical specialties as of March 2009: allergy and immunology, anesthesiology, colon and rectal surgery, dermatology, emergency medicine, family medicine, internal medicine, neurological surgery, nuclear medicine, obstetrics and gynecology, ophthalmology, orthopedic surgery, pediatrics, physical medicine and rehabilitation, plastic surgery, psychiatry and neurology, radiology, surgery, thoracic surgery, and urology. |
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
environment. However, no evidence exists to predict how physicians would respond to changes in CE financing.
In the absence of evidence, the committee assumes that physicians could maintain participation in activities similar to the ones in which they currently participate (e.g., a hybrid of low-cost, journal-based CME with occasional participation in higher quality, higher cost activities) without paying more out of pocket.
Although the question of what would happen were commercial support removed is critically important, no empirical evidence exists to date to support or refute hypotheses of how commercial supporters would respond. A determination cannot be made of whether the costs of an ideal system would be greater than the costs of the current system.
Funding is unequal and unstable across all health professions. The lack of data about the financing of CE is alarming because data are needed to determine how to invest most efficiently in CE. Current methods of financing cannot support a comprehensive, evidence-based learning system that promotes high quality, high value health care that is free from conflict of interest. It is likely, however, that sufficient funding exists within the current structure to support better learning. If better aligned with overall efforts to improve the quality of care, continuing professional development could maintain professional competence and help prepare professionals to improve patient outcomes in the absence of industry funding. Significant spending that currently supports less effective activities could and should be redirected toward more effective activities to counter the significant losses from conflicted funding sources.
REFERENCES
ABMS (American Board of Medical Specialties). 2009. ABMS maintenance of certification. http://abms.org/Maintenance_of_Certification/ABMS_MOC.aspx (accessed April 23, 2009).
ACCME (Accreditation Council for Continuing Medical Education). 2006. ACCME essential areas and their elements: Updated decision-making criteria relevant to the essential areas and elements. Chicago, IL: ACCME.
———. 2008. ACCME annual report data 2007. http://www.accme.org/dir_docs/doc_upload/207fa8e2-bdbe-47f8-9b65-52477f9faade_uploaddocument.pdf (accessed January 16, 2009).
AMA (American Medical Association). 2006. The physician's recognition award and credit system: Information for accredited providers and physicians. Edited by the American Medical Association. http://www.ama-assn.org/ama1/pub/upload/mm/455/pra2006.pdf.
———. 2008. State medical licensure requirements and statistics, 2008. Chicago, IL: AMA Press.
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
ANCC (American Nurses Credentialing Center). 2009. ANCC accreditation application manual. http://www.nursecredentialing.org/ContinuingEducation/Accreditation/AccreditationProcess.aspx (accessed July 15, 2009).
Blumenthal, D. 2004. Doctors and drug companies. New England Journal of Medicine 351(18):1885-1890.
Brennan, T. A., D. J. Rothman, L. Blank, D. Blumenthal, S. C. Chimonas, J. J. Cohen, J. Goldman, J. P. Kassirer, H. Kimball, J. Naughton, and N. Smelser. 2006. Health industry practices that create conflicts of interest: A policy proposal for academic medical centers. Journal of the American Medical Association 295(4):429-433.
Brosky, J. A., and R. Scott. 2007. Professional competence in physical therapy. Journal of Allied Health 36(2):113-118.
Coogle, L. 2008. Perspectives on continuing education from providers and funders. Presentation to the Committee on Planning a Continuing Health Care Professional Education Institute, December 11. Washington, DC: North American Association of Medical Education and Communication Companies.
Cooke, M., D. M. Irby, W. Sullivan, and K. M. Ludmerer. 2006. American medical education 100 years after the Flexner report. New England Journal of Medicine 355(13):1339-1344.
Davis, D., M. Evans, A. Jadad, L. Perrier, D. Rath, D. Ryan, G. Sibbald, S. Straus, S. Rappolt, M. Wowk, and M. Zwarenstein. 2003. The case for knowledge translation: Shortening the journey from evidence to effect. British Medical Journal 327(7405):33-35.
DeAngelis, C. D., and P. B. Fontanarosa. 2008. Impugning the integrity of medical science: The adverse effects of industry influence. Journal of the American Medical Association 299(15):1833-1835.
Grossman, J. 1998. Continuing competence in the health professions. American Journal of Occupational Therapy 52(9):709-715.
IOM (Institute of Medicine). 2009. Conflict of interest in medical research, education, and practice. Washington, DC: The National Academies Press.
Mazmanian, P. E. 2009. Commercial support of continuing medical education in the United States: The politics of doubt, the value of studies. Journal of Continuing Education in the Health Professions 29(2):81-83.
Mazmanian, P. E., D. E. Moore, R. M. Mansfield, and M. P. Neal. 1979. Perspectives on mandatory continuing medical education. Southern Medical Journal 72(4):378-380.
McCartney, M. 2004. The giving game: Do the freebies that doctors get from drugs companies affect the treatment they pick for patients? Guardian (May 25):10.
Michigan State Medical Society Committee on CME Accreditation. 2009. Policy & procedure manual (a guide to the accreditation process). East Lansing, MI: Michigan State Medical Society.
Miller, S. H., J. N. Thompson, P. E. Mazmanian, A. Aparicio, D. Davis, B. Spivey, and N. Kahn. 2008. Continuing medical education, professional development, and requirements for medical licensure: A white paper of the conjoint committee on continuing medical education. Journal of Continuing Education in the Health Professions 28(2):95-98.
NASW (National Association of Social Workers). 2003. NASW standards for continuing professional education. http://www.socialworkers.org/practice/standards/NASWContinuingEdStandards.pdf (accessed July 15, 2009).
Peck, C., M. McCall, B. McLaren, and T. Rotem. 2000. Continuing medical education and continuing professional development: International comparisons. British Medical Journal 320:432-435.
Suggested Citation:"3 Regulation and Financing." Institute of Medicine. 2010. Redesigning Continuing Education in the Health Professions. Washington, DC: The National Academies Press. doi: 10.17226/12704.
×
Peterson, E. D., K. M. Overstreet, J. N. Parochka, and M. R. Lemon. 2008. Medical education and communication companies in CME: An updated profile. Journal of Continuing Education in the Health Professions 24(8):205-219.
PhRMA (Pharmaceutical Research and Manufacturers of America). 2008. Code on interactions with healthcare professionals. Washington, DC: PhRMA.
Podolsky, S. H., and J. A. Greene. 2008. A historical perspective of pharmaceutical promotion and physician education. Journal of the American Medical Association 300(7):831-833.
Relman, A. S. 2001. Separating continuing medical education from pharmaceutical marketing. Journal of the American Medical Association 285(15):2009-2012.
Saxton, M. 2009. A view from industry: The foundations of future commercial support and a call for action. Journal of Continuing Education in the Health Professions 29(1):71-75.
Smith, J. L., R. M. Cervero, and T. Valentine. 2006. Impact of commercial support on continuing pharmacy education. Journal of Continuing Education in the Health Professions 26(4):302-312.
Steinbrook, R. 2005. Commercial support and continuing medical education. New England Journal of Medicine 352(6):534-535.
———. 2008. Financial support of continuing medical education. Journal of the American Medical Association 299(9):1060-1062.
United States Senate Committee on Finance. 2007. Committee staff report to the chairman and ranking member: Use of educational grants by pharmaceutical manufacturers. Washington, DC: U.S. Government Printing Office.
Source: https://nap.nationalacademies.org/read/12704/chapter/5
0 Response to "How to Cite the Institute of Medicine Redesigning Continuing Education in the Health Professions"
Post a Comment